 News
News  Market Data
Market Data  Discover
Discover 
Support: 888-992-3836
Copyright © 2023 InvestorsHub Inc.





Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
Anytime. What I found pretty interesting is this part that is considered part of the 150 day assessment. It may be the reason for the extra 700k pages and Les’ statement about the fall.
Access Consortium work-sharing procedures: If you are considering a National Application for either a new active substance, a biosimilar product, or a new indication application, then the MHRA invites you to consider submission via an Access Consortium work-sharing procedure. These procedures allow simultaneous submission to the UK, Australia, Canada, Singapore and/or Switzerland. Potential advantages to companies include:
Simultaneous submission for access to multiple markets.
Streamlined process: Internationally coordinated review to reduce duplication/burden. Joint, consolidated lists of questions, capturing the assessment of all agencies.
Predictability: Work-sharing and peer-review between agencies, with pre-determined joint international milestones.
Competitive timetables: Standard procedure of 180 days (excluding stop-clocks).
Flexibility: Module 1 will be different between jurisdictions, while minor differences in Module 2-5 may also be accepted. Separate sovereign decisions at end of procedure
Opportunity to make a contribution to innovation in the area of regulation.
Thanks, Astavakra, for your kind correction based on excellent DD! The CHM meeting is where advisers decide how to advise the MHRA about approvals. So decisions on approval will likely lag behind the CHM meeting dates I gave in my former posts.
From Astavakra's DD: from ChatGBT:
In the UK, the Commission on Human Medicines (CHM) is responsible for advising the Medicines and Healthcare products Regulatory Agency (MHRA) on matters relating to the safety, efficacy, and quality of medicines. One of the key responsibilities of the CHM is to make recommendations regarding Marketing Authorisation Applications (MAAs) for new medicines.
Strange how you are changing the topic.
Speaking at an event celebrating efforts to tackle AMR at the Royal Society on Thursday, William called for international and cross-sector co-operation regarding the issue.
Both the King and the prince’s wife, the Princess of Wales, have undergone treatment for cancer in recent months which can weaken the immune system and leave patients prone to infection.
And we have 3 paid 🐀S, trying all kinds of trash for cash posting maneuvers to make the right, wrong,,,,
Bunch of lost in life translation to humanity & scam wannabes.
One might even be a stray dog on learning curve!!
Sniff away !!!
A slight distinction: It's my understanding from reading about the CHM on the UK.Gov site, that they act in an advisory roll only. They can recommend approval, but the approval still rests with MHRA.
From the site:
The Commission on Human Medicines was established in October 2005. Its functions are set out in regulation 10 of the Human Medicines Regulations 2012 (SI 2012/1916).
Our responsibilities
We’re responsible for:
advising on applications for both national and European marketing authorisations
considering further representation against our provisional advice in respect of national applications
advising on the need for, and content of, risk management plans for new medicines
advising on the impact of new safety issues on the balance of risks and benefits of licensed medicines - eg adding warnings, restricting or suspending use of a medicine
advising the licensing authority on changes to legal status of marketing authorisations
In the UK, the Commission on Human Medicines (CHM) is responsible for advising the Medicines and Healthcare products Regulatory Agency (MHRA) on matters relating to the safety, efficacy, and quality of medicines. One of the key responsibilities of the CHM is to make recommendations regarding Marketing Authorisation Applications (MAAs) for new medicines.
The CHM does hold regular meetings, typically on a monthly basis, where they discuss various issues, including the assessment of MAAs. During these meetings, the CHM reviews detailed reports and data on new medicines to determine whether they meet the necessary standards for approval. Their recommendations are then considered by the MHRA, which makes the final decision on whether to grant a marketing authorisation.
Thus, the CHM plays a crucial role in the decision-making process for MAAs during their monthly meetings by providing expert advice and recommendations based on their evaluations of the medicines in question.
https://www.gofundme.com/f/bos-brain-cancer-journey
One thing to note is Bo refused to take chemo and he is back in the States after having his booster DcVaxL doses from UK and is resting well.
Filiper is right that chemo kills recurrent brain cancer patients and is interfering in the efficacy of DcVaxL; glad Bo didn’t take it.
exwannabe,
This is a very correct assessment which is why I did not say it would not be approved, however, no one wants to use a product with a potential to be less effective as a consequence of different type of administration. The broad range of other adverse events were also different and some categories strikingly so which is likely because of different types of administration.
I get what you are saying about non inferiority range but as you have seen with L, improvements have been made since the Phase 3 and those are translating into improved outcomes not worse or technically non inferior.
The other issue is that if something like these results came out for L there would be a whole slew of attacks by the bears about this. Just sayin; ). Best wishes.
rizona - It would appear that this latest Harrington Order adds muscle to serving and discovery capabilities.
Worth reposting imo. Subsequent trials and review of outcome data has shown no benefit for 43% cancer drugs which were fast tracked for approval. Where DCVAX is concerned, all data leads to Rome, past and current. The paid shills sure missed a lot of opportunities to prove they know anything about approvable trial outcomes.
https://www.cbsnews.com/news/cancer-drugs-remain-unproven-years-after-fda-accelerated-approval-study/
The court can sanction a side for willful disclosure violations. It is uncommon.
Kam8 - The broad leeway granted to this patent is breathtaking. Effects on immune modulation is clearly unaccompanied by what those specific modulators would be. Unless I missed something? This patent is worth billions imo.
Correct. But BioHarm needs everyone to think it is approved.
>>The FDA (the U.S. Food and Drug Administration) has not approved personalized neoantigen
peptides, Hiltonol® or Montanide® a as a treatment for any disease.
>>The FDA (the U.S. Food and Drug Administration) has not approved personalized neoantigen
peptides, Hiltonol® or Montanide® a as a treatment for any disease. It is an investigational
drug being developed for use in the treatment of metastatic melanoma.
The FDA has approved Nivolumab (Opdivo®) and Ipilimumab (Yervoy™) as a treatment option for
this disease.
The FDA has approved Ipilimumab administered intravenously as a treatment option for this
disease.
The FDA has not approved Ipilimumab administered subcutaneously (under the skin) as a
treatment for any disease.
https://www.mycancergenome.org/content/clinical_trials/NCT03929029/
>>The drug was also under development for the treatment of brain tumor, anaplastic astrocytoma, anaplastic oligoastrocytoma, oligodendroglioma, glioblastoma multiforme, poxviridae infections, west nile virus infections, japanese encephalitis, dengue fever, yellow fever, st louis encephalitis, murray valley, orthopox virus infections, banzai viruses, smallpox, severe acute respiratory syndrome (SARS), acute myeloid leukemia, myelodysplastic syndrome, chronic myelomonocytic leukemia (CMML) and influenza.
The company’s pipeline products include hiltonol plus dendritic cell vaccine and hiltonol (Poly-ICLC) plus temodar.
https://www.pharmaceutical-technology.com/data-insights/poly-iclc-oncovir-metastatic-adenocarcinoma-of-the-pancreas-likelihood-of-approval/?cf-view
Kam8 - The broad leeway granted to this patent is breathtaking. Effects on immune modulation is clearly unaccompanied by what those specific modulators would be. Unless I missed something? This patent is worth billions imo.
Gus, I just updated that post with one date change. Doesn't change the options, though.
I agree 100%. Praying for full discloser and a trial by jury to bring true justice to the MMs and all
involved. The jury can decide the outcome and how a corrupt team of MMs and others suppressed
NWBO and deprived many cancer patients who could have benefited from the approval of DCVax years ago, IMPO.
The fact that you are calling it the SAME treatment shows how little you know and/or how disingenuous you are. Please don't do that.
Says nothing really. No survival stats or testimonials?
>>They state a 70% response rate, which is a bit ambiguous.
Folks, I got a date wrong on the third approval possibility, so I'm reposting it with the correction, thanks to VL. But it doesn't change hypothetical approval meeting dates.
What are the possibilities that DCVax-L will be approved for new GBM and recurring GBM at one of the next four meetings of the UK’s CHM (Commission on Human Medicines).
They meet on these dates:
May 30-31
June 27-28
July 25-26
Aug. 29-30.
But which is most likely approval day?
Many have already discounted May 30-31, but I think it’s still possible. First, It fits with our submission deadline date of Dec. 25, 2023. May 25 is exactly 150 days from this deadline, but it’s a Saturday, so if UK’s CHM wants to move quickly on DCVax-L, it makes sense that they would approve it at 149 days, rather wait another month for when the commission meets next. Secondly, we received a “validation confirmation” date on May 7th, which just happens to be 2 days before we hit the 80-day completion of Phase 1 of the regulatory process, if you believe the clock started on Dec. 20 when we submitted our application.
But we have since learned that the clock starts when we receive “validation”. Our application passed validation on Jan. 24th, then our validation was “confirmed" on March 7th. The two different validations reported in the quarterly have created some confusion and speculation. I think there is a possibility that the second validation may represent when our application completed Phase I where we received NO request for info from CHM, which means NO need to stop the 150-day clock. Confirm means to check again. That fits with the idea that the first validation was quicker and less thorough and was followed by a more complete examination of the MAA, which ended in the March 7th confirmation and perhaps the end of Phase I. This hypothesis only works if we assume CHM ignored their very late (IMO) Jan. 24 validation and moved quickly to study our MAA.
The second possible CHM meeting on June 27-28 coincides with the first validation date of Jan. 24. 150 days out from Jan. 24 is actually June 22, another Saturday and 5 days before the start of this meeting. If we follow the 150-day law to the letter and believe there is no clock stop for answering questions, then this is the likeliest time to expect the UK to make a decision on our application.
The third possible CHM meeting date, July 25-26, somewhat aligns with the possibility that the clock started when our validation was “confirmed” on March 7th. 150 days out from that confirmation is actually August 4, a Sunday. If CHM members wanted to move along our MAA, they could choose to make their decision on July 25-26, which is 6 days before the 150-day review ends which includes a weekend.
If they decide not to make a decision on our MAA a week early, they would have to wait almost a month until their next meeting on Aug. 29-30. I don’t see that happening unless they are trying to give our automated system another month to complete validation.
None of these dates address the possibility that NWBO may need to stop the clock to respond to a request for information letter from the UK. If this happens it could add 60 or even 120 days to the approval process. I think a clock stop at this point is unlikely, given the comments by Les and in the quarterly. Both were very bullish comments. NWBO has been very cagey about appearing bullish because so many negative shorts have attacked the company and even reported them to regulators when they’ve committed lesser infractions. If the clock started on Dec. 25 or on Jan. 24, in both cases, we would have completed the 80-day phase I long before the time we received the quarterly on May 10 and heard Les speak on May 9. If we accept the March 7th date for when the 150-day clock began, we would have been about 2 weeks before completion of Ph. 1 I believe the rules state that companies receive a request for info only after Ph 1 is complete. I think it’s unlikely Les would have been so bullish as to state “no news is good news” and the quarterly would have told us they had not changed a thing in our MAA if they knew the potential clock-stopping news was still in the future.
Of course, all of this assumes CHM doesn't set a special meeting for NWBO's application.
Yes, they call it the protocol + treatment, which is SOC + and or the vaccine , and or Cap and or any other supplementary drugs deemed appropriate.
All treatment combination variants is determined by the assigned German Consultant.
They state a 70% response rate, which is a bit ambiguous.
But what is good, is that each treatment is adaptive, patient specific, and no doubt adapted to fit the budget of the individual health Tourist.
But for the vaccine alone, the cost is as I stated.
Poly-ICLC is already an approved drug
We promote Hiltonol® as an experimental viral mimic and broad activator of innate and adaptive immunity. We have partnered extensively with both commercial companies and academic institutions.
Oncovir manufactues GMP grade clinical material for use in approved regulatory settings and preclinical material suitable for preclinical and scientific exploration
Great catch, VMLG17! I counted weeks so many times trying to get it right, I thought my eyes would cross! Anyway, I think both those two CHM dates could still be in play. August 4 is 150 days after the March 7th date when we received our Validation Confirmation. That's six days after the July meeting and 25 days before the August 29-30 meeting. I'll correct it and print again in case anyone wants to reprint it for fams and friends.
Thanks Beartrap
Appreciate the work that went into this post.
Best
Perhaps the royal family should make a contribution from their 88B net worth to NICE to cover treatments...
Talk about waste...How much is the Sovereign Grant each year?
Between the Sovereign grant, assets from the properties, and the crown estate, the royal family is paid up to $1.2 billion. Wouldn't this money be better spent if some of it went to NICE's budget?...
Sure seems like a lot of money to keep the tabloids employed.
Thx beartrap, but I think there's typo: 150 days from March 7 is August 4.
I’m glad you agree on what he said. I’m sure they have a list of drugs the royalty review prior to approval. Protocol of course.
Do the German's tout any actual success rate?
The fact that you are calling it the SAME treatment shows how little you know and/or how disingenuous you are. Please don't do that.
Also, don't bother to respond. I won't reply, as just typing this out I consider a waste of my time, and better judgement
WOW!!!
Why cant the court hold the defendants in contempt for stalling, preventing and hiding pertinent data from the plaintiff?
The judge needs to come down hard and these mofo's
Nice work, thanks.
Re:Beartrap12
My family and I have held NWBO since mid 2018 and have added some along the way.
I am new on this board as far as posting, however, I do follow the board and truly appreciate your insights.
Regards
During Prince William latest trip He said: “There is an urgent need for new measures to access new and existing vaccines, diagnostics and medicines.
QL300, I want to send out a special thanks to you for posting this link to the MHRA's website on the 150-day review. I should have looked it up myself before, but didn't. Everyone should go through this url! I hope I copied it properly. If not, go back to QL 300's post.
[url][/url][tag]https://www.gov.uk/guidance/guidance-on-150-day-assessment-for-national-applications-for-medicines[/tag]
During Prince William latest trip He said: “There is an urgent need for new measures to access new and existing vaccines, diagnostics and medicines.
I say the next meeting May 30-31. You have less than 2 weeks to cover.
Someone always sell the shares in last minute
Thank you, IinvestK. Your name is new to me and I see you have only a few recent comments on NWBO blog. Hope you stay positive despite the armies of naysayers here!
Thank you, Gus. I actually wrote it for my large Beartrap family and plan to send it to them soon. That's why I didn't use many shortcut letters, but spelt things out!
Its okay to wish things will happen next week...But to hope they will is just going to disappoint you....I don't expect any news until mid June...
Patience is the name of the game...For sure, I wanted big news months ago, right now approval is all that matters.
I’m glad you have finally moved to the position that DCVAX will be approved. The only question is when. Your time scale should be in days or seconds if you want a big number. It’s submitted with no RFI’s.
Good boy Nemesis - Snif away, chaise your own tail, and make your day posting trash for cash..
What are the possibilities that DCVax-L will be approved for new GBM and recurring GBM at one of the next four meeting of the UK’s CHM (Commission on Human Medicines).
Beartrap12
Your detailed analysis regarding MHA possible approval time lines are truly appreciated.
Thank you for the time, effort and detailed analysis you provide related to NWBO.
Thank You for this write up of the possible approval dates!!
It certainly clears up many questions.
I will be sending your write up to all of my People invested here.
And there are many -
Your post is so detailed it should be placed on top of this blog/ message board
Thaks Again
>>>First Canadian to get a life-extending brain cancer treatment administered in Canada, even though it’s not yet approved" (DCVax)<<<
Hopefully, as many Brits are learning, it’s cheaper to receive dendritic cell cancer treatment when arranged direct with German treatment centres, who manufacture their own vaccines on site, rather that going through either Advent or London Hospitals ! (About 6th of the cost.)
At that level of cost, it’s worth the punt for the patient and their family, unlike many people here in the UK have found out, after spending £250,000,!it didn’t make a shit of difference to the OS.
I’m certain that the NICE,at some point, will demand to know why this cost disparity exists between Germany and the UK ?
What are the possibilities that DCVax-L will be approved for new GBM and recurring GBM at one of the next four meeting of the UK’s CHM (Commission on Human Medicines).
They meet on these dates:
May 30-31
June 27-28
July 25-26
Aug. 29-30.
But which is most likely approval day?
Many have already discounted May 30-31, but I think it’s still possible. First, It fits with our submission deadline date of Dec. 25, 2023. May 25 is exactly 150 days from this deadline, but it’s a Saturday, so if UK’s CHM wants to move quickly on DCVax-L, it makes sense that they would approve it at 149 days, rather wait another month for when the commission meets next. Secondly, we received a “validation confirmation” date on May 7th, which just happens to be 2 days before we hit the 80-day completion of Phase 1 of the regulatory process, if you believe the clock started on Dec. 20 when we submitted our application.
But we have since learned that the clock starts when we receive “validation”. Our application passed validation on Jan. 24th, then our validation was “confirmed" on March 7th. The two different validations reported in the quarterly have created some confusion and speculation. I think there is a possibility that the second validation may represent when our application completed Phase I where we received NO request for info from CHM, which means NO need to stop the 150-day clock. Confirm means to check again. That fits with the idea that the first validation was quicker and less thorough and was followed by a more complete examination of the MAA, which ended in the March 7th confirmation and perhaps the end of Phase I. This hypothesis only works if we assume CHM ignored their very late (IMO) Jan. 24 validation and moved quickly to study our MAA.
The second possible CHM meeting on June 27-28 coincides with the first validation date of Jan. 24. 150 days out from Jan. 24 is actually June 22, another Saturday and 5 days before the start of this meeting. If we follow the 150-day law to the letter and believe there is no clock stop for answering questions, then this is the likeliest time to expect the UK to make a decision on our application.
The third possible CHM meeting date, July 25-26, somewhat aligns with the possibility that the clock started when our validation was “confirmed” on March 7th. 150 days out from that confirmation is actually July 29, a Monday. If CHM members wanted to move along our MAA, they could choose to make their decision the weekend before completion of the 150-day time table and hear it on July 25-26.
If they decide not to make a decision on our MAA a weekend early, they would have to wait almost a month until their next meeting on Aug. 29-30. I don’t see that happening unless they are trying to give our automated system another month to complete validation.
None of these dates address the possibility that NWBO may need to stop the clock to respond to a request for information letter from the UK. If this happens it could add 60 or even 120 days to the approval process. I think a clock stop at this point is unlikely, given the comments by Les and in the quarterly. Both were very bullish comments. NWBO has been very cagey about appearing bullish because so many negative shorts have attacked the company and even reported them to regulators when they’ve committed lesser infractions. If the clock started on Dec. 25 or on Jan. 24, in both cases, we would have completed the 80-day phase I long before the time we received the quarterly on May 10 and heard Les speak on May 9. If we accept the March 7th date for when the 150-day clock began, we would have been about 2 weeks before completion of Ph. 1 I believe the rules state that companies receive a request for info only after Ph 1 is complete. I think it’s unlikely Les would have been so bullish as to state “no news is good news” and the quarterly would have told us they had not changed a thing in our MAA if they knew the potential clock-stopping news was still in the future.
Of course, all of this assumes CHM doesn't set a special meeting for NWBO's application.
Someone always sell the shares in last minute to make sure it close red every single day. It has happened so many times.
This way retail won't get confused. Disciples have put a lot into name recognition.
I wonder if they'll have security to keep Feuerstein out?? I hope he makes a documentary.
#dcvax $nwbo #gbm @GovCanHealth @braincancercan
— Peter Davis (@peter_brit) May 18, 2024
"First Canadian to get a life-extending brain cancer treatment administered in Canada, even though it’s not yet approved" (DCVax)
The federal government estimates that on average 27 people a day in this country are diagnosed with… pic.twitter.com/e67wAUq1Wg
|
Followers
|
1625
|
Posters
|
|
|
Posts (Today)
|
66
|
Posts (Total)
|
692477
|
|
Created
|
02/02/05
|
Type
|
Free
|
| Moderators XenaLives sentiment_stocks CaptainObvious Poor Man - Doc logic JerryCampbell | |||
![]()
“Now this is not the end. It is not even the beginning of the end. But it is, perhaps, the end of the beginning.”
~ Winston Churchill

Stylized Dendritic Cell featured on NWBO board since 2015

- Dr. Linda Liau, PhD, MBA, Professor and Chair, Department of Neurosurgery, David Geffen School of Medicine at UCLA
Clinical Trials
DCVax®-L to Treat Newly Diagnosed GBM Brain Cancer (NCT00045968) - Phase III (Double Blind)
UK (MHRA): DCVax-L to Treat Newly Diagnosed GBM Brain Cancer (EudraCT#) 2011-001977-13
DE (Germany - PEI): DCVax-L to Treat Newly Diagnosed GBM Brain Cancer (EudraCT#) 2011-001977-13
Expanded Access Protocol for GBM Patients with Already Manufactured DCVax®-L Who Have Screen-Failed Protocol 020221 (NCT02146066) (Expanded Access)
Safety and Efficacy Study of DCVax-Direct in Solid Tumors (NCT01882946) - Phase I/Phase II (Open Label)
UK Clinical Trials - Study of a Drug (DCVax®-L) to Treat Newly Diagnosed GBM Brain Cancer
EU Clinical Trials for DCVax-L - Phase III
Dendritic Cell Vaccine for Patients with Brain Tumors (NCT01204684) - Phase II - at UCLA - Randomized (Open Label) testing DCVaccine with Resiquimod and DC Vaccination with Adjuvant polyICLC
Pembrolizumab and a Vaccine (ATL-DC) for the treatment of Surgically Accessible Recurrent Glioblastoma - Phase 1 (NCT04201873)
Dendritic Cell-Autologous Lung Tumor Vaccine (DCVax-L) and Nivolumab in Treating Patients with Recurrent Glioblastoma - Phase 2 (NCT03014804)
Dendritic Cell Therapy for Brain Metastases From Breast or Lung Cancer (NCT0368765) - Phase 1 - Collaborator: Mayo Clinic
Announcement of DCVax-L and Anti-PD-1 Monoclonal Antibody (Pembrolizumab) for Patients with Liver Metastases of Primary Colorectal Carcinoma Phase 2 Trial - November 17, 2016 - University Medical Center (UMC) of the Johannes Gutenberg University of Mainz
Cognate Bioservices - Owned by Charles River Labs
Website
Company Contact Info
Investor Relations:
Les Goldman (Company) (202) 841-7909 lgoldman@nwbio.com
Sign up for Northwest email list here (hit the subscribe to email list button in the lower right)
Company Headquarters
4800 Montgomery Lane, Suite 800, Bethesda, MD 20814 (240) 497-9024
NW Bio is developing cancer vaccines designed to treat a broad range of solid tumor cancers more effectively than current treatments, and without the side effects of chemotherapy drugs. NW Bio’s proprietary manufacturing technology enables them to produce its personalized vaccine in an efficient, cost-effective manner. NW Bio has a broad platform technology for DCVax dendritic cell-based vaccines.
Their lead product, DCVax-L, is currently in a 331-patient Phase III trial for patients with newly diagnosed Glioblastoma multiforme (GBM), the most aggressive and lethal brain cancer. This trial is currently underway at 69 locations thoughout the United States, Germany and the United Kingdom. NW Bio has also conducted a Phase I/II trial with DCVax-L for late stage ovarian cancer together with the University of Pennsylvania.
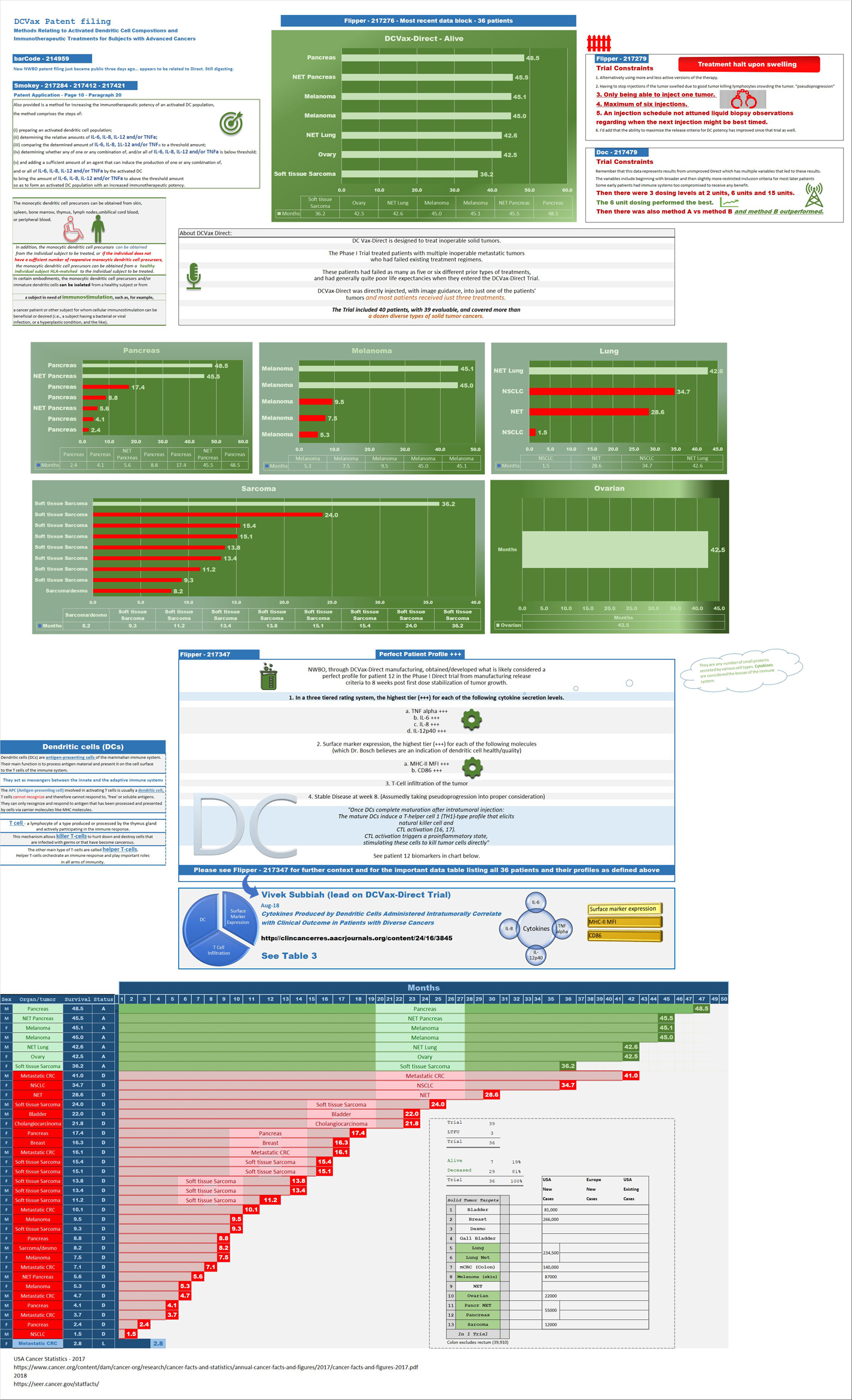
Their second product, DCVax-Direct, is currently in a 60-patient Phase I/II trial for direct injection into all types of inoperable solid tumor cancers, with trials currently being conducted at both MD Anderson Cancer Center in Texas, as well as Orlando Health in Florida.
They previously received clearance from the FDA for a 612-patient Phase III trial with its third product, DCVax-Prostate, for late stage prostate cancer.
DCVAX Survival Stories & Testimonials
Alice - Metastic Merkel Cell patient from Florida - ASCO 2018
Brad Silver - GBM patient from Huntington Beach, California - ASCO 2018
Sarah Rigby - GBM patient from Hong Kong - ASCO 2018
Kristyn Power - daughter of GBM patient from Canada - ASCO 2018
Kat Charles - GBM patients from UK - ASCO 2018 - as related by her husband Jason (Kat's Cure)
Prospective patients may contact NW Bio at patients@nwbio.com
UCLA Jamil Newirth DCVax-Patient Video - 2015
Allan Butler Video - National Geographic Vice President - DCVax-Direct patient from Phase 1 Trial with Pancreatic Cancer
NWBO - Patients Sunday Dennis and Jami Newirth - Enrolled at UCLA - Vimeo, Uploaded approx. May 2015
NWBO - Vaccine Helps Keep Brain Cancer Patient Alive (Jennifer Sugioka) - NBC Channel 4, Southern California, February 24, 2015
NWBO - National Geographic's Allan Butler Stage IV Pancreatic Patient using DCVax-Direct at MD Anderson
NWBO GBM Brain Cancer Survival Story of Mark Pace

Presentations

UCLA Agreements
Prostrate
DCVax-Phase II
DCVax-Booster
Upcoming Events
Videos
Linda M. Liau, MD, PhD, MBA - April 24, 2019 at University of Washington, Neurosciences Institute
| Volume | |
| Day Range: | |
| Bid Price | |
| Ask Price | |
| Last Trade Time: |





